
Ear Pain Is Not Always an Ear Problem | A Recurrent Cervical-Related Ear Pain Case
MRI normal. Ear examination normal.
But the pain kept returning for 15 years.
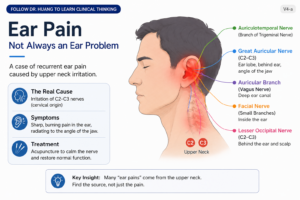
Ear Pain Is Not Always an Ear Problem
A Clinical Reflection on a Recurrent Ear Pain Case
A Patient with 15 Years of Recurrent Ear Pain
Recently, I saw a patient who had been suffering from recurrent left-sided ear pain for nearly fifteen years.
In the early years, the attacks occurred only once or twice a year. Each episode lasted for one or two hours before settling spontaneously, so the patient simply tolerated it.
However, over the last two years, the attacks became more frequent. Eventually, they started happening once or twice a week. The patient described the pain as sharp, burning, and deep inside the ear canal. During severe episodes, the pain also radiated toward the angle of the jaw.
He had already seen specialists and undergone MRI examination. No significant abnormality was found. Pain medication provided temporary relief at best, but the attacks continued to recur.
At that point, the patient felt he needed more than temporary symptom control. He wanted to understand why the pain kept returning.
Why This Did Not Fully Fit Trigeminal Neuralgia
At first glance, trigeminal neuralgia seemed like a reasonable possibility.
But clinically, the pattern did not completely fit.
Typical trigeminal neuralgia usually presents as brief electric shock-like pain triggered by touch, speaking, chewing, or facial stimulation. This patient’s pain behaved differently. The episodes lasted much longer, the burning sensation was more prominent, and the pain distribution extended beyond the classic trigeminal territory.
Most importantly, the pain was centered deep in the ear and extended toward the jaw angle rather than the face itself.
That detail became important later.
The Examination Finding That Changed My Thinking
During examination, one finding stood out clearly: significant tenderness around the left C2–C3 cervical region.
This immediately changed the direction of my thinking.
The ear is not supplied by a single nerve. In fact, it is one of the most neurologically complex sensory regions in the body.
Its sensory input involves multiple nerves, including:
- the auriculotemporal branch of the trigeminal nerve
- the great auricular nerve
- the auricular branch of the vagus nerve
- small facial nerve branches
- the lesser occipital nerve
Because these sensory systems overlap and converge centrally, the brain does not always precisely distinguish which pathway is generating abnormal input.
As a result, patients often describe a generalized “deep ear pain,” even when the original irritation may arise elsewhere.
Why the Jaw Angle Was Important
In this patient, the pain consistently radiated toward the angle of the jaw.
This is clinically significant because the great auricular nerve — originating from C2 and C3 — supplies sensation not only to the ear region, but also to the area around the jaw angle.
That made me consider the possibility that the ear itself was not the primary problem.
Instead, the pain may have originated from irritation within the upper cervical sensory system, particularly around the C2–C3 region, and then projected into the ear through shared sensory pathways.
In other words:
the ear may simply be where the pain is felt, not where the problem begins.
The Response After Treatment
The patient was extremely afraid of acupuncture because he had never experienced it before.
During the first session, he even told me:
“I’ll close my eyes. Just do it.”
After treatment, something interesting happened.
The severe ear pain did not return. Instead, he reported only a mild itchy sensation deep inside the ear canal.
Clinically, this transition from pain to itch-like sensation can sometimes indicate reduced neural hypersensitivity. The abnormal sensory discharge appears to calm down, leaving behind a milder residual sensation.
At this stage, I do not believe this case represents a straightforward “great auricular nerve injury.” There is no obvious sensory loss, persistent numbness, or evidence of structural nerve damage.
It appears more consistent with a cervical-related sensory irritation syndrome involving the upper cervical network and its associated ear sensory pathways.
Why Cases Like This Matter
Cases like this remind us of something important:
Pain location does not always identify pain origin.
Many chronic pain conditions cannot be fully understood by looking only at the organ or body part where symptoms appear.
Sometimes the real issue lies within the sensory network behind the symptoms — the way the nervous system processes, amplifies, and projects sensation.
This may also explain why some patients continue to suffer despite normal scans and normal examinations.
The absence of visible structural disease does not necessarily mean the absence of dysfunction.
What I Will Continue to Observe
At this point, the most important thing is not simply whether the pain disappears immediately.
What matters more is:
- whether the attacks become less frequent
- whether the duration shortens
- whether the nervous system becomes less reactive over time
These changes often tell us more about recovery than short-term symptom relief alone.
This case is still evolving, and continued observation will be important.
But it already highlights an increasingly important clinical principle:
Ear pain is not always an ear problem.
Sometimes, the true source lies higher up in the sensory system.
Internal Links
Booking CTA
If you are experiencing ongoing ear pain, facial pain, or unexplained nerve-related symptoms, you can book an appointment here:
 中文微信:nzacupunctureclinic
中文微信:nzacupunctureclinic
Leave a reply