A “Shoulder Strain” Patient Later Found to Have Spinal Cord Hemorrhage Requiring Emergency Surgery
Shoulder & Upper Back Pain Case Study | Dr Huang Chinese Medicine Clinic Auckland
Many dangerous diseases do not look dangerous in the early stage.
This case has stayed in my mind for many years because at the beginning it looked like a very ordinary shoulder and upper back strain.
But later it developed into:
- spinal cord hemorrhage
- sudden paralysis of both legs
- emergency surgery
- long-term rehabilitation
I am sharing this case not because it was a “successful treatment.”
Actually, cases that teach the most are often the ones that are:
- atypical
- misleading
- unexpectedly worsening later
1. Initial Presentation
The patient was a middle-aged man.
The symptoms started while he was pulling tree branches during gardening work at home. He suddenly felt pain around the right shoulder and upper back.
At first, both the patient and others thought it was:
- a simple strain
- muscular injury
- overuse from pulling
However, the pain quickly became unusually severe.
The patient described:
- waking up at night because of pain
- constant severe shoulder and upper back pain
- pain much stronger than a normal strain
Later he came to Dr Huang Chinese Medicine Clinic for acupuncture treatment after being referred by a friend.
2. The First Signs That Raised My Suspicion
During the first examination, several things did not fit a typical muscle strain pattern.
When pressure was applied around the neck, the pain did not stay localised.
Instead, it radiated:
- into the upper back
- into the shoulder
- even into the chest
This pattern already suggested neurological involvement.
A typical muscular shoulder strain usually presents with:
- local tenderness
- movement pain
- muscle pulling discomfort
But this patient showed:
- wide radiation pattern
- severe night pain
- nerve-like pain
- major sleep disturbance
At that stage I already began suspecting:
👉 this might not simply be a musculoskeletal strain.
I even told the patient directly:
“This does not look like a normal strain. It looks more like nerve pain.”
Later, the patient sent me a text message saying:
“The treatment for my nerves pain on my back and chest.”
This message later became an important reminder that both the patient and I already recognised unusual neurological features early in the process.
3. Response After Initial Treatment
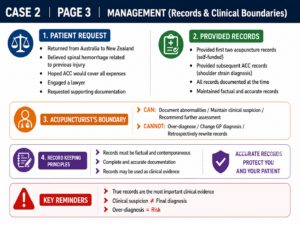
The patient received two acupuncture treatments.
After treatment:
- symptoms improved slightly
- but recovery remained limited
- severe night pain continued
This further increased my concern.
Normally, if acute shoulder strain is treated correctly:
- symptoms usually improve quickly
- night pain gradually reduces
- muscle recovery becomes obvious within days
But this patient’s recovery pattern did not behave like an ordinary strain.
4. ACC Reality and Clinical Boundaries
Later the patient saw his GP.
Because the patient believed the symptoms began after pulling tree branches, the GP created an ACC claim and diagnosed the case as shoulder strain / sprain.
This reflects a very common reality in clinical practice.
As acupuncturists, we may have:
- clinical observations
- suspicions
- red flag concerns
But we are not the final medical diagnosticians.
The ACC injury diagnosis is established by the GP.
Therefore:
- I could not independently change the diagnosis
- I could not formally diagnose spinal cord disease
- I could not label it as neurological hemorrhage
So later ACC documentation continued under the shoulder strain pathway.
However, clinically, I continued to feel:
👉 “This case does not behave like a normal shoulder strain.”
I also advised the patient to seek further medical review.
5. Sudden Deterioration in Australia
After several treatments, the patient travelled to Australia because his symptoms had slightly improved.
He planned to continue treatment after returning to New Zealand.
Months later, he suddenly contacted me again.
He requested his previous treatment records and asked whether I could provide documentation related to neurological injury.
Only then did I learn what had happened.
While in Australia, his condition suddenly deteriorated.
He developed:
- weakness in both legs
- inability to walk
- bladder and bowel dysfunction
He was taken to hospital urgently.
CT and MRI later revealed:
👉 cervical spinal cord hemorrhage.
Emergency surgery was performed immediately.
Fortunately, after prolonged rehabilitation, the patient eventually recovered well without permanent paralysis or bowel/bladder complications.
6. Looking Back at the Case
Looking back now, I believe the patient may already have had:
- early spinal cord pathology
- vascular abnormality
- inflammatory neurological disease
- or early hemorrhagic changes
before he first attended for acupuncture treatment.
The gardening incident may not have been the true cause.
More likely, it acted as:
- a trigger
- a provoking event
- or something that accelerated an existing underlying condition
Because a simple muscular strain cannot easily explain:
- severe night pain
- extensive neurological radiation
- sudden paralysis later
- spinal cord hemorrhage on MRI
7. My Biggest Reflection From This Case
One regret has stayed with me for years.
If the patient had accepted further investigation earlier — especially cervical MRI imaging — the outcome may possibly have been very different.
Even during the early stage, the case already showed several warning signs inconsistent with ordinary strain injuries:
- severe night pain
- widespread nerve-like radiation
- pain radiating into chest and upper back when neck pressure was applied
- unusually slow recovery
- symptoms far exceeding normal muscular injury patterns
These signs already suggested:
👉 possible deeper neurological involvement.
But at that time:
- the patient believed it was a strain
- the GP had established an ACC shoulder strain claim
- no major neurological deficits had appeared yet
- the patient travelled overseas after three treatments
So the case continued moving through the “ordinary injury” pathway.
Only later did MRI reveal spinal cord hemorrhage.
If MRI had been performed earlier, perhaps it may have allowed:
- earlier diagnosis
- earlier neurosurgical assessment
- earlier intervention
- possible prevention of severe deterioration
Of course, this is retrospective reflection.
The real difficulty is this:
👉 many dangerous diseases do not initially appear dangerous.
That is why:
👉 Clinical suspicion is often more important than treatment technique itself.
8. Documentation and Legal Issues
This case later created a very difficult medico-legal situation.
Because of:
- prolonged hospitalisation
- surgery
- inability to work
- major medical costs
the patient hoped ACC would cover expenses related to the Australian treatment.
However, ACC argued that the spinal cord hemorrhage was unrelated to the original injury.
The patient later engaged a lawyer and asked me to support the claim.
My earliest clinical notes did document:
- neurological radiation pain
- suspicion of neurological involvement
- recommendation for further assessment
However, later ACC documentation still followed the GP shoulder strain diagnosis.
This case deeply reinforced for me:
👉 clinical documentation is extremely important.
Especially for:
- private patients
- first consultations
- unusual pain presentations
Many practitioners become less careful when ACC is not directly involved.
But when serious complications arise later:
👉 retrospective memory becomes unreliable.
Only the original clinical records can truly reflect what happened at the time.
9. My Clinical Principle
I did not rewrite history afterward.
I only provided:
- the original records
- the original findings
- the original symptoms
Because I believe the greatest medico-legal risk is not simply misdiagnosis.
It is:
👉 failing to document properly, or rewriting records afterward.
As practitioners, we can:
- document abnormal findings
- maintain clinical suspicion
- recommend further investigation
- warn patients about risk
But we should not retrospectively change records based on later outcomes.
10. Clinical Insights
This case left several very important lessons for me.
Severe Night Pain Must Raise Suspicion
Especially when combined with:
- night waking pain
- widespread radiation
- nerve-like symptoms
- recovery patterns inconsistent with normal strain injuries
These situations require consideration of:
- neurological disease
- spinal cord pathology
- hemorrhage
- inflammation
- tumour-related causes
When the Pattern Does Not Match the Diagnosis, Think Deeper
Pain radiating into the chest, back, and nerve pathways does not fit ordinary shoulder strain logic.
Sometimes the diagnosis itself needs to be questioned.
Mature Clinical Experience Is Not About “Treating Everything”
It is about recognising:
👉 “This case does not behave like a normal case.”
That awareness is often more important than technical skill.
Documentation Is Part of Clinical Safety
Clinical records are not simply administrative tasks.
They preserve:
- real symptoms
- real examination findings
- real clinical thinking
Today, AI tools can help organise records efficiently.
But the final responsibility still belongs to the clinician.
Why Choose Dr Huang Chinese Medicine Clinic
At Dr Huang Chinese Medicine Clinic, we do not only focus on where the pain is.
We also pay attention to:
- pain behaviour
- radiation pathways
- recovery patterns
- neurological red flags
- whether the disease process fits normal clinical logic
Because many dangerous diseases do not look dangerous at the beginning.
Dr Huang’s Clinical Red Flag Cases
- “Shoulder Strain” Later Found to Have Spinal Cord Hemorrhage
- “Frozen Shoulder” for Months — But It Was ALS
- chronic shoulder pain, it is a benign tumor
- Calf Pain? It Turned Out to Be Deep Vein Thrombosis (DVT)
- A Long-Term “Upper Back Pain” Patient Later Found to Have Significant Coronary Artery Disease
- Seeking Treatment for Hearing Loss,I think it is a brain tumour
- Shoulder and Arm Numbness? It Turned Out to Be Syringomyelia
- Leg Cramps for Years? It Turned Out to Be a Brain Meningioma
- She Thought It Was Just Bloating, but it be diagnosed an ectopic pregnancy.
- A “Trigeminal Neuralgia” Patient Whose Real Problem Turned Out to Be a Dental Abscess | Auckland
- A “Chronic Sciatica” Patient Who Was Eventually Diagnosed with Lung Cancer and Brain Metastasis
CTA
👉 Severe night pain, widespread radiation pain, or unusually slow recovery?
👉 The problem may not be a simple muscle strain.
👉 Book Online: https://drwin.co.nz/online-booking/
 中文微信:nzacupunctureclinic
中文微信:nzacupunctureclinic
Leave a reply