
Why Complex Shoulder Pain Cannot Have Only One Diagnosis
The purpose of this series is not simply to show how a patient was treated.
What I hope to share is the clinical reasoning behind each case.
In daily practice, difficult cases rarely have a single explanation. The challenge is not only making the diagnosis, but understanding which problem is causing the patient’s symptoms today, which affects function, and which may require long-term management.
This shoulder injury illustrates exactly that.
The Shoulder Injury Was Only the Beginning
The patient injured her right shoulder at work.
Initially the pain was mild. She was still able to continue working and did not think the injury was serious.
Later, a co-worker performed a very deep massage around the shoulder and neck. During the massage she immediately felt sharp pain. That evening the pain became dramatically worse. She could barely move the shoulder, could not sleep because of severe pain, and pain medication provided little relief.
Looking back, I believe the severe deterioration may not have been caused by the original injury alone. It is possible that aggressive massage further irritated already injured tissues and increased neural sensitivity.
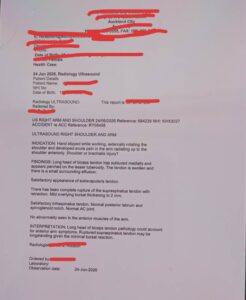
The Ultrasound Showed Structural Damage
Ultrasound later demonstrated:
- Complete supraspinatus tendon rupture with tendon retraction
- Medial subluxation of the long head of the biceps tendon
- Local tendon swelling and inflammation
Many clinicians might immediately conclude that the torn rotator cuff explained all of the patient’s pain.
I did not.
The Pain Behaved More Like Nerve Pain
When I first examined her, the pattern of pain did not resemble typical tendon pain.
She had severe resting pain.
She had night pain.
She described sharp, radiating pain rather than simple movement pain.
Palpation of the scalene muscles reproduced the same pain she experienced around the shoulder and upper arm.
Several structures around the thoracic outlet also reproduced her symptoms.
These findings suggested that neural mechanosensitivity was playing a major role.
The First Treatment Confirmed My Thinking
During the first treatment I did not focus on the torn supraspinatus tendon.
Instead, I treated the highly sensitive tissues around the thoracic outlet, particularly the scalene muscles.
Immediately after treatment her pain reduced by approximately 30%.
That night she was finally able to sleep.
The following day she returned saying her pain had improved by approximately 70–80%.
This rapid improvement suggested that the major driver of her severe pain was neural irritation rather than the chronic tendon tear itself.
Once the Pain Improved, Another Problem Became Obvious
At the second visit, the patient’s main complaint had changed.
She was no longer overwhelmed by pain.
Instead, she noticed catching during shoulder elevation.
At this stage, I believed the swollen and partially unstable long head of the biceps tendon had become the dominant problem.
Inflammation and tendon swelling likely contributed to the catching sensation during movement.
As swelling gradually resolves, shoulder mechanics may continue to improve.
An Old History Completed the Puzzle
Further questioning revealed an important detail.
Around 2019–2020 she had experienced another episode of severe shoulder pain.
It settled within several days without treatment.
However, ever since then she had always felt that her right shoulder was “not quite the same.”
Occasionally it felt weak.
Occasionally it caught during movement.
Occasionally it simply did not feel normal.
Combined with the ultrasound finding of tendon retraction, I suspect that the supraspinatus rupture may have occurred years earlier rather than during this recent workplace injury.
A Three-Layer Diagnosis
This patient demonstrated three different clinical layers.
Layer One – Neural Pain
Thoracic outlet neural mechanosensitivity explained the severe resting pain, night pain and radiating symptoms.
Layer Two – Functional Mechanical Dysfunction
Swelling and instability of the long head of the biceps tendon explained the catching sensation during shoulder movement.
Layer Three – Structural Pathology
The chronic supraspinatus tendon rupture explained the long-term reduction in shoulder stability that had been present for several years.
Each layer contributed differently to the patient’s presentation.
Treatment Also Required Three Layers
The treatment plan followed the same principle.
First, reduce neural sensitivity so the patient could sleep, move, and regain confidence.
Second, reduce inflammation around the long head of the biceps tendon and improve dynamic shoulder function.
Third, recognise that the chronic supraspinatus tendon rupture remained a structural issue. The patient should be assessed by an orthopaedic shoulder specialist to determine whether further management, including surgery, may be appropriate.
Treating today’s pain does not necessarily resolve every underlying structural problem.
Dr Huang’s Clinical Reflection
This case reinforced an important lesson.
Many clinicians naturally think in a one-to-one model:
One symptom.
One diagnosis.
One treatment.
Real clinical practice is rarely that simple.
Complex patients often present with several pathological processes occurring simultaneously.
One explains today’s pain.
Another explains movement dysfunction.
Another determines long-term prognosis.
If we fail to separate these different layers, our diagnosis becomes oversimplified and our treatment may target the wrong problem.
The human body also reminds us of something else.
A complete tendon rupture does not always mean complete loss of function.
This patient had likely lived with a chronic supraspinatus rupture for years while continuing normal work and daily activities.
The shoulder compensated through other muscles, particularly the deltoid and remaining rotator cuff muscles.
Imaging tells us what structures are damaged. Clinical reasoning tells us which problem is actually producing the patient’s symptoms today.
That is the message I hope to share through this series.
Frequently Asked Questions
Does a torn rotator cuff always require surgery?
Not necessarily. Treatment depends on age, functional demands, symptoms, chronicity of the tear, and specialist assessment.
Can someone have a complete tendon tear without severe disability?
Yes. Many patients develop excellent muscular compensation and maintain useful shoulder function despite chronic rotator cuff tears.
Why didn’t Dr Huang treat the rotator cuff first?
Because the patient’s pain pattern suggested neural mechanosensitivity was the primary pain generator at that stage. The clinical examination supported this reasoning.
What is the main lesson from this case?
Complex shoulder pain should not be explained by a single diagnosis. Understanding the different pathological layers leads to better clinical decisions and more appropriate treatment.
Medical Disclaimer
This article is intended for health education and to share clinical reasoning. It is not intended as personal medical advice, diagnosis, or treatment.
Every patient is different. Similar symptoms do not necessarily indicate the same condition. Anyone experiencing persistent pain or functional limitation should seek assessment from an appropriately qualified healthcare professional.
Book an Appointment
If you have persistent shoulder pain, limited movement, night pain, or recurrent shoulder injuries, a comprehensive clinical assessment is often more valuable than relying on imaging findings alone.
Book an appointment with PhD Win Acupuncture Clinic to receive an individual assessment and personalised treatment plan.
 中文微信:nzacupunctureclinic
中文微信:nzacupunctureclinic
Leave a reply