A Patient Arrived with a Diagnosis, But Not Necessarily the Answer
Several years ago, a middle-aged European man came to my clinic seeking acupuncture treatment for severe facial pain.
Unlike many patients, he did not come without a diagnosis. His GP had already diagnosed him with trigeminal neuralgia, and he simply wanted pain relief.
His symptoms had been present for three to four months.
Initially, he believed the problem was coming from his teeth, so he visited a dentist. Dental examinations and imaging failed to identify any obvious dental pathology. He was then referred back to his GP, who felt that trigeminal neuralgia was the most likely diagnosis and prescribed medication for nerve pain.
At first, the medication helped.
However, during the week before I saw him, everything changed.
The pain became progressively worse.
He was waking multiple times during the night.
The medication was no longer providing meaningful relief.
He knew something was wrong.
A friend suggested acupuncture, and that was how he eventually arrived at my clinic.
Why I Began to Doubt the Diagnosis
One habit I have developed over many years of clinical practice is that I never assume a previous diagnosis is automatically correct.
Every patient is re-examined from the beginning.
The diagnosis belongs to someone else.
The clinical judgment must be my own.
During examination, I noticed that the right side of his face was unusually sensitive.
Further testing revealed similar hypersensitivity over the right side of his scalp.
He also reported headaches, and there was marked tenderness around the Fengchi (GB20) region.
At that point, a question immediately came to mind.
If this were simply primary trigeminal neuralgia, why was there an obvious sensory abnormality?
Typical neuralgia causes pain.
It does not necessarily alter sensory perception itself.
Yet this patient demonstrated clear sensory hypersensitivity.
This suggested that the nerve was not simply producing pain. It was being irritated or affected by an underlying process.
I therefore began to suspect that this was not primary trigeminal neuralgia at all, but rather a secondary neuralgia.
Once that possibility entered the picture, the focus of the consultation changed completely.
I was no longer asking whether he had trigeminal neuralgia.
I was asking why he had trigeminal neuralgia.
The Enlarged Lymph Node That Changed Everything
I continued examining his neck and jaw.
There I found the most important physical finding of the entire consultation.
A large swelling was present beneath the right side of his jaw.
It was approximately the size of a walnut and was significantly tender to palpation.
The right side of his neck was also visibly swollen.
At the time, I believed it was an enlarged lymph node.
Importantly, this was not a mildly enlarged lymph node.
This was substantial.
Now the clinical picture became much more concerning.
Why would a patient have:
- Trigeminal nerve hypersensitivity?
- Occipital nerve involvement?
- A markedly enlarged lymph node?
- Neck swelling?
These findings pointed toward a common underlying cause.
Inflammation immediately became a major consideration.
The source of the inflammation, however, remained unclear.
Could it be a dental infection?
A deep tissue infection?
Herpes zoster?
Or something else entirely?
I did not know the answer.
What I did know was that this case could not be explained simply by the label “trigeminal neuralgia.”
The Three Recommendations I Gave
Based on the findings, I gave the patient three recommendations.
First, he needed further investigation. I advised him to return to his GP and pursue additional diagnostic testing. Given the involvement of both trigeminal and occipital nerve regions, CT or MRI imaging of the head and neck should be considered.
Second, because waiting times in New Zealand’s healthcare system can be lengthy, acupuncture could be used to help control symptoms while awaiting further assessment.
Third, if the pain continued to worsen or the condition progressed, he should not wait.
He should go directly to Auckland Hospital Emergency Department.
Two Days Later He Was Admitted to Hospital
The patient followed the third recommendation.
He went directly to the emergency department.
The process moved quickly.
Assessment.
Investigation.
Admission.
Surgical planning.
Within a short period of time, he was already in hospital.
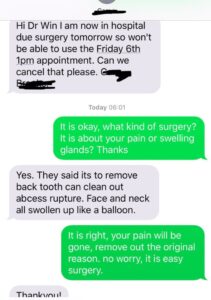
Shortly afterward he sent me a text message explaining that he had been admitted and was scheduled for surgery the next day.
When I asked what type of surgery was planned, he replied that doctors had identified the source of the problem.
A posterior tooth would need to be removed.
An abscess would need to be drained and cleaned.
He also wrote:
“Face and neck all swollen up like a balloon.”
At that moment, the entire case finally made sense.
Final Diagnosis: Dental Abscess
The hospital ultimately diagnosed a retromolar dental abscess.
Treatment included:
- Extraction of the affected tooth
- Surgical drainage and debridement
- Infection management
- Hospital observation
Looking back, neither the trigeminal neuralgia nor the occipital neuralgia was entirely wrong.
The mistake was assuming that neuralgia itself was the final diagnosis.
In reality, the neuralgia was only the consequence.
The infection was the true cause.
The dental abscess produced inflammation, which irritated nearby neural structures and ultimately generated months of facial pain.
This was, in essence, a case of secondary neuralgia caused by infection.
Dr Huang’s Clinical Reflection
This case reinforced an important lesson.
Patients often arrive with a diagnosis.
That does not mean they arrive with the correct answer.
One of the most important responsibilities of a clinician is not simply accepting a diagnosis, but continually testing whether that diagnosis still explains the patient’s condition.
When symptoms become more severe, medication becomes less effective, new signs appear, and the overall picture becomes more complex, it may be necessary to start the diagnostic process again from the beginning.
In this case, what changed the patient’s outcome was not acupuncture.
It was recognising that the clinical picture no longer behaved like simple trigeminal neuralgia.
Many dangerous conditions are not missed because nobody knows the diagnosis.
They are missed because everyone continues believing the original diagnosis long after it no longer fits.
Sometimes the most important intervention is not a treatment.
Sometimes it is recognising that:
“This is no longer the same disease we thought it was.”
Book Online
 中文微信:nzacupunctureclinic
中文微信:nzacupunctureclinic
Leave a reply