Shoulder Pain That Was Not a Shoulder Problem
Many chronic shoulder pain cases are not truly shoulder joint problems.
This patient was a man I treated last year.
At first glance, his symptoms looked relatively ordinary:
- right shoulder pain;
- pain around the axillary region;
- symptoms for more than one year;
- severe pain;
- but surprisingly little restriction in shoulder movement.
Because of the ongoing pain, he had already undergone:
- specialist assessment;
- MRI;
- ultrasound;
- physiotherapy;
- acupuncture;
- massage treatment.
Some minor abnormalities were mentioned, but nobody found a major explanation.
Yet clinically, one thing was clear:
👉 The patient was getting progressively worse.
That alone already suggested this was unlikely to be a simple shoulder disorder.
The Symptom That Immediately Raised My Suspicion
The most important detail was not actually the shoulder pain itself.
During consultation, the patient described a very unusual symptom.
He said:
👉 Every time he strained during bowel movement, the pain would shoot upward from the lower spine all the way toward the neck.
He described it as:
- severe;
- electric-like;
- difficult to tolerate;
- forcing him to stop straining.
This was extremely important clinically.
Because ordinary shoulder disorders do not behave like this.
Typical shoulder pain usually relates to:
- movement;
- lifting;
- reaching;
- tendon loading.
But this patient’s pain pattern involved:
👉 spinal pressure-related radiating pain.
At that moment, I already began thinking:
👉 This may not be a shoulder problem at all.
Further Neurological Examination Revealed Multiple Red Flags
I then performed a more detailed neurological examination.
Several abnormal findings immediately stood out.
1. Abnormal Upper Limb Reflexes
The first major red flag was:
👉 abnormal reflexes in the right upper limb.
Simple shoulder conditions usually do not cause reflex changes.
Reflex abnormalities suggest:
👉 neurological pathway involvement.
2. Hand Muscle Wasting
More importantly, he already showed visible wasting around:
- the first dorsal interosseous region;
- intrinsic hand muscles;
- thenar area.
This indicated:
👉 long-term nerve compression or neurological dysfunction.
Simple shoulder inflammation does not cause intrinsic hand muscle wasting.
3. Declining Fine Motor Control
I asked him to perform:
- finger opposition;
- pinch testing;
- fine coordination movements.
These movements were already noticeably impaired.
This meant:
👉 the problem had progressed beyond pain alone.
Neurological function itself was being affected.
My Clinical Localization Thinking
Based on:
- reflex abnormalities;
- hand muscle wasting;
- impaired fine motor function;
- unusual pain behavior;
- spinal radiating pain during straining;
I strongly suspected pathology around:
👉 the C7–T1 junction.
In other words:
👉 the cervicothoracic transition zone.
At that stage, I also began suspecting:
👉 a space-occupying lesion rather than a simple inflammatory condition.
Possible considerations included:
- tumor;
- nerve sheath lesion;
- compressive pathology;
- other space-occupying process.
At that time, I did not know exactly what it was.
But I knew clearly:
👉 MRI was urgently required.
Why This Case Was Clinically Important
This case highlights one of the most important mistakes clinicians often make:
👉 “Shoulder pain = shoulder disease.”
True neurological reasoning is different.
The key question is:
👉 Where is the lesion actually located?
This patient’s symptoms no longer matched ordinary shoulder pathology.
Especially:
- worsening progression;
- neurological findings;
- intrinsic muscle wasting;
- spinal radiation during straining;
all pointed toward deeper neurological involvement.
The problem was not in the shoulder itself.
The shoulder pain was simply:
👉 the surface presentation of a neurological lesion.
MRI Result and Surgical Outcome
After hearing my concerns, the patient became understandably anxious.
He arranged MRI shortly afterward.
The result was dramatic.
After MRI, the hospital directly admitted him for surgery.
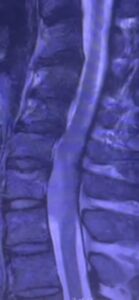
The scan revealed:
👉 a space-occupying lesion around the C7–T1 region.
Fortunately, postoperative pathology later confirmed:
👉 a benign tumor.
After surgery:
- the severe pain improved rapidly;
- neurological symptoms became much better.
However:
- muscle wasting;
- nerve recovery;
- hand function restoration;
still required prolonged rehabilitation.
The Most Important Clinical Lesson
The most important part of this case was not:
👉 “guessing the tumor correctly.”
The real lesson was:
👉 Persistent conditions that never follow normal recovery patterns always deserve re-evaluation.
If:
- simple treatment works;
- physiotherapy improves things;
- symptoms fluctuate normally;
then the condition may indeed be musculoskeletal.
But if a patient becomes:
- progressively worse;
- increasingly neurological;
- increasingly atypical;
then clinicians must stop asking:
“What treatment should I use?”
and instead ask:
👉 “Why is this case not behaving normally?”
Key Red Flags in This Case
1. Progressive worsening
Not fluctuating.
👉 Continuously worsening.
2. Pain severity disproportionate to movement restriction
Very severe pain.
But relatively preserved shoulder movement.
3. Pain triggered by straining during bowel movement
A major neurological red flag.
4. Reflex abnormalities
Suggesting neurological involvement beyond local shoulder structures.
5. Intrinsic hand muscle wasting
Indicating long-standing neural compression.
6. Declining fine motor function
Showing actual neurological dysfunction progression.
Shoulder Pain Is Sometimes a Neurological Problem
This case also reflects something broader in clinical medicine.
Many practitioners focus only on:
- the pain location;
- MRI wording;
- tendon findings;
- local inflammation.
But clinically, persistent pain often involves:
- neurological pathways;
- spinal cord compression;
- nerve root dysfunction;
- central irritation patterns.
This is why basic neurological examination matters enormously.
Even for acupuncturists.
Because many patients we see every day present with:
- pain;
- numbness;
- weakness;
- coordination changes;
- movement dysfunction.
These problems overlap heavily with:
- neurology;
- orthopedics;
- rehabilitation medicine.
One Reflection That Stayed With Me
Many clinicians believe:
👉 keeping the patient for ongoing treatment means success.
But over the years, I increasingly feel:
👉 knowing when NOT to continue treating in the same direction is true clinical maturity.
This patient later trusted me deeply.
Not because I performed complicated treatment.
But because:
👉 he felt somebody finally understood the real nature of his illness.
Patients often do not remember how many needles you used.
They remember:
👉 whether you truly understood what was happening.
Clinical Insight
Many dangerous neurological diseases initially appear ordinary.
Persistent shoulder pain that:
- keeps worsening;
- behaves abnormally;
- develops weakness;
- causes muscle wasting;
- changes reflexes;
should never automatically be labeled as “frozen shoulder” or “simple shoulder strain.”
Sometimes the real problem is not the shoulder at all.
Why Choose PhD Win Acupuncture Clinic
At PhD Win Acupuncture Clinic, we do not only focus on where the pain is.
We also assess:
- neurological patterns;
- reflex changes;
- muscle wasting;
- movement dysfunction;
- radiating symptoms;
- Red Flag signs;
- whether the clinical pattern truly matches the diagnosis.
Many serious conditions initially appear deceptively ordinary.
Clinical suspicion is often more important than treatment technique itself.
Dr Huang’s Clinical Red Flag Cases
- “Shoulder Strain” Later Found to Have Spinal Cord Hemorrhage
- “Frozen Shoulder” for Months — But It Was ALS
- chronic shoulder pain, it is a benign tumor
- Calf Pain? It Turned Out to Be Deep Vein Thrombosis (DVT)
- A Long-Term “Upper Back Pain” Patient Later Found to Have Significant Coronary Artery Disease
- Seeking Treatment for Hearing Loss,I think it is a brain tumour
- Shoulder and Arm Numbness? It Turned Out to Be Syringomyelia
- Leg Cramps for Years? It Turned Out to Be a Brain Meningioma
- She Thought It Was Just Bloating, but it be diagnosed an ectopic pregnancy.
- A “Trigeminal Neuralgia” Patient Whose Real Problem Turned Out to Be a Dental Abscess | Auckland
- A “Chronic Sciatica” Patient Who Was Eventually Diagnosed with Lung Cancer and Brain Metastasis
CTA
👉 Persistent shoulder pain getting worse?
👉 Hand weakness or muscle wasting developing?
👉 Symptoms not matching ordinary shoulder problems?
The issue may not actually be inside the shoulder.
Book Online:
 中文微信:nzacupunctureclinic
中文微信:nzacupunctureclinic
Leave a reply