
Case 1|Acute Right Thoracolumbar Pain: From Sharp Back Pain to Cough Pain — A Four-Tier Diagnostic Pathway
① Case Background
A 46-year-old female developed sudden, severe right thoracolumbar pain one week ago while bending forward to pick up an item in the kitchen.
The pain extended from the right costal margin down to the iliac crest. The patient described it as “right lower back and flank pain.”
Typical features:
-
Pain significantly worsened with coughing, sneezing, or deep breathing
-
Pain increased with thoracolumbar movement
② Four-Tier Clinical Reasoning
🔵 Tier 1: Symptom-Level Interpretation — The Trap of “Muscle Strain”
At first glance, this appears to be a typical “acute back strain” scenario:
-
Sudden onset after bending
-
Localized tenderness
-
Patient feels she “twisted her back”
Thus, many clinicians and patients naturally assume:
muscle strain / muscle spasm / soft-tissue injury
However, this explanation fails to answer key questions:
-
Why does coughing, sneezing, or deep breathing immediately worsen the pain?
A muscle strain alone does not produce sharp, cough-induced pain.
👉 Staying only at the muscular level easily leads to diagnostic misdirection.
🟡 Tier 2: Functional / Neurological Interpretation — This Is Nerve Root Irritation
Clinically, the question should shift from “Where does it hurt?” to
“When does it hurt the most?”
Three hallmark symptoms stand out:
-
Coughing pain
-
Sneezing pain
-
Deep-breathing pain
These strongly suggest nerve root irritation.
Physical examinations further confirmed this:
-
Hyperalgesia in the right T10–T12 dermatomes
-
Paraspinal tenderness at T10–T12, with referred pain to the patient’s symptomatic region
Together, these findings point to:
Intercostal neuralgia / thoracic nerve root irritation
This is no longer a muscular issue.
👉 The nervous system is signaling distress.
This tier marks the shift from “muscle thinking” to “neurogenic thinking.”
🟠 Tier 3: Structural / Mechanistic Interpretation — What Is Irritating the Nerve Root?
After confirming nerve root involvement, the next essential question is:
“Why is the nerve root irritated?”
Several examination clues provided the answer:
-
Distinct paraspinal tenderness at T10–T12
-
Restricted mobility in the same segments
-
Immediate reduction in cough pain after facet joint mobilization
These findings strongly support:
Thoracic facet joint dysfunction / capsular entrapment → irritation of the corresponding nerve root → intercostal neuralgia
The diagnosis thus progresses from “what hurts” to
👉 “what mechanism is creating the pain.”
🔴 Tier 4: Deep Structural Interpretation — Why Did Facet Dysfunction Occur?
The deeper question is not
“Which joint is misaligned?”
but rather:
“Why is this patient prone to facet joint locking?”
Common underlying contributors include:
-
Prolonged sitting and forward-bending postures → thoracolumbar stiffness / flat-back posture
-
Mild scoliosis or asymmetric spinal loading
-
Insufficient core stability
-
The thoracolumbar junction’s inherent nature: low stability + limited mobility
In such a structural environment,
even a simple forward-bending movement can trigger facet locking → nerve root irritation → acute sharp back pain, cough-induced pain, and abdominal radiation.
This tier reminds us:
The acute episode is the result; long-standing structural imbalance is the true cause.
③ Treatment Strategy
The management approach is straightforward:
1. Remove the source of nerve root irritation
-
Mobilize the thoracolumbar facet joints
-
Release tissues potentially impinging or tethering the nerve root
2. Reduce protective muscular guarding
-
Acupuncture or manual techniques to relax hypertonic muscles
-
Interrupt the protective spasm cycle
3. Restore normal joint mobility
-
Guide the patient through gentle flexion, extension, and side-bending
-
Reestablish proper joint biomechanics
After one treatment, the patient’s severe pain significantly reduced, and coughing no longer triggered sharp pain, confirming that the nerve root irritation was relieved.
④ Key Clinical Insight
Back pain should not be evaluated only by “where it hurts.”
Once coughing pain appears, nerve root irritation must be considered.
Following the pathway of neurogenic pain leads to identifying facet dysfunction, spinal imbalance, and deeper structural contributors.
Case 2|Left Testicular Pain: A Psoas Chain–Induced Neural Traction Trap
① Case Background
The patient is a Kiwi male.
He has experienced left testicular discomfort for approximately 13 years, with significant worsening over the past two years.
Main symptoms:
-
Dull ache and aching sensation in the left testicle
-
A feeling of scrotal heaviness or “dragging”
-
Mild discomfort in the left inguinal region
-
Standing or prolonged walking aggravates symptoms
-
Lying down relieves symptoms
-
NSAIDs (ibuprofen, Voltaren) provide relief
-
Antibiotics have no effect
He was previously severely obese (around 130 kg) and later lost nearly 50 kg through surgery and fat-reduction procedures.
His current weight is around 90 kg.
The patient believed his symptoms might be related to a vasectomy he underwent when younger or possibly to varicocele.
One week ago, after receiving treatment at my clinic, he happily reported that he experienced several days without any pain, confirming that our diagnostic direction was correct.
② Four-Level Thinking Analysis
🔵 Level 1: Symptom Layer — Is “testicular pain” really coming from the testicle?
Typical testicular pain is often misattributed to:
-
Epididymitis
-
Varicocele
-
Post-vasectomy pain syndrome
However, this case presents several contradictions:
-
No tenderness of the testicle itself
-
No redness, swelling, or warmth
-
Antibiotics completely ineffective
-
NSAIDs effective
-
Significant improvement after a single structural treatment
All of these suggest:
👉 The problem is NOT within the testicle itself.
🟡 Level 2: Functional / Neural Layer — A classic pattern of neural traction pain
The clinical triad:
-
Dull ache
-
Dragging sensation
-
Mild inguinal discomfort
strongly suggests genitofemoral nerve traction pain.
Symptom behavior:
-
More activity → worse
-
Rest / lying down → relief
-
NSAIDs effective
-
Antibiotics ineffective
This pattern indicates:
👉 Pain arises from neural tension and traction, not infection.
🟠 Level 3: Structural / Mechanistic Layer — The psoas muscle is the true source
Three key clinical findings:
**① Deep abdominal palpation of the psoas showed:
Hypertrophy, hardness, and pain rated 6/10 on the affected side (vs 1–2/10 on the healthy side)**
→ Indicates long-term psoas tension and inflammatory thickening.
② Positive Thomas Test
→ Clear evidence of psoas shortening.
③ Audible snapping during hip flexion/extension (“snapping psoas”)
→ A classic sign of abnormal tendon glide.
These structural abnormalities create a clear chain:
Psoas hypertrophy and tightness
⬇
Traction on L1–L2 nerve roots
⬇
Irritation of the genitofemoral nerve
⬇
Manifestation as “pseudo testicular pain”
👉 The pain originates from the psoas chain, not the testicle.
🔴 Level 4: Deep Structural Layer — Obesity, rapid weight loss, and collapse of mechanical chains
This is the most critical layer in this case.
The patient had long-standing severe obesity (~130 kg).
During obesity:
-
Excess abdominal mass
-
Chronic anterior pelvic tilt
-
Psoas overactivation to stabilize the spine
-
Gradual development of chronic hypertrophy and shortening
Then he underwent rapid weight loss of nearly 50 kg.
Deep mechanical consequences of rapid weight loss:
1) The psoas, already chronically hypertrophied, does NOT regain normal elasticity simply because weight decreases
Muscle architecture remains shortened and tight.
2) Trunk stability decreases abruptly
With reduced abdominal mass,
the psoas must take on even more stabilizing work
→ continuous over-tightening
→ increased neural traction
3) Neural structures become more exposed and sensitive
Soft-tissue buffering decreases after weight loss
→ the genitofemoral nerve becomes more vulnerable to traction
→ symptoms worsen
This explains why symptoms have intensified over the past two years, forming a classic pattern of:
Obesity → chronic psoas overload
⬇
Hypertrophy + shortening
⬇
Rapid weight loss → instability
⬇
Increased neural traction
⬇
Pseudo testicular pain
③ Treatment Strategy
Goal: Release the psoas chain traction on the genitofemoral nerve.
Key steps:
1) Deep psoas release (the most critical step)
-
Abdominal deep-pressure technique
-
Needling into the psoas access points
-
Improve tendon glide and reduce muscle tone
2) L1–L2 facet mobilization
Reduce nerve-root tension.
3) Gentle release at the inguinal nerve-exit zone
Assist in reducing neural traction.
4) Establish psoas relaxation and hip-extension training
Shift the psoas from a “compensatory pattern” back to a functional pattern.
After a single treatment session, symptoms improved dramatically, repeatedly confirming the correctness of the diagnostic chain.
④ Clinical Insight
Many cases of “testicular pain” do NOT originate from the testicle itself,
but from neural traction caused by the psoas chain.
Understanding structural chains is the key to eliminating the pain.
#——————————————————————————————————————————————#
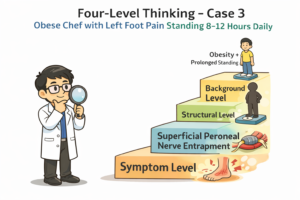
Case 3 | Left Foot Pain (2 Weeks): Peripheral Nerve Entrapment in the Context of Obesity and Prolonged Standing
1. Case Background
The patient is a 30-year-old Chinese female, working as a chef, with a body weight of 95 kg.
She presented with left foot pain lasting for approximately two weeks.
Pain characteristics:
-
Pain occurs during walking and is intermittent
-
One episode of significant exacerbation, during which she was unable to move for approximately two hours
-
Pain is not constant
-
No clear history of ankle sprain, fall, or direct trauma
On the surface, this appears to be a common presentation of “foot pain.” However, the pain pattern does not fully match typical ankle sprain or simple local soft-tissue strain, warranting further analysis.
2. Four-Level Thinking Analysis
🔵 Level 1 | Symptom Level – What are the symptoms?
At the symptom level, the presentation seems straightforward:
-
Pain localized to the left foot
-
Pain related to walking
-
Short duration of symptoms
At this level, it is most easily categorized as:
-
Local foot strain, gout, or small joint inflammation
-
Ankle or soft tissue problem, ankle instability
However, in Four-Level Thinking, Level 1 focuses on recording phenomena rather than drawing conclusions, leaving room for deeper analysis.
🟡 Level 2 | Functional / Neurological Level – How does the pain behave?
Further examination revealed several key findings:
-
Hyperalgesia in the painful area
-
Subjective abnormal sensations described by the patient (e.g., “feels thick,” “feels different from normal”)
-
Severe, sharp pain that does not resemble simple pressure pain or muscle strain
These features suggest:
👉 The pain is more consistent with neurological dysfunction, rather than a primary muscle or joint problem.
At this level, diagnostic thinking shifts from “structural pain” to neuropathic pain.
🟠 Level 3 | Structural / Mechanism Level – Which structure is responsible?
After excluding restricted ankle joint motion and obvious joint pathology, and based on neurological localization:
-
Sensory disturbance and pain were mainly distributed over the distal lower leg and dorsum of the foot
-
Marked tenderness was noted at Xuanzhong (GB39)
-
Ankle muscle strength was symmetrical bilaterally, making common peroneal nerve involvement unlikely
Considering nerve distribution and physical findings, the diagnosis gradually focused on:
Superficial peroneal nerve entrapment
Palpation over common entrapment sites of the superficial peroneal nerve reproduced localized pain, completing the symptom–structure verification loop.
🔴 Level 4 | Background / Load Level – Why did this problem occur in this person?
This is the most critical level in this case.
The patient is approximately 175 cm tall and weighs about 95 kg, which is clearly above the ideal weight range.
She works as a chef and stands for approximately 8–12 hours per day, placing her lower limbs under sustained load.
Under this background, several important biomechanical factors are present:
-
Excess body weight significantly increases continuous load on the lower limbs
-
Prolonged standing maintains the lateral lower-leg fascia in a state of chronic high tension
-
The sliding space of the nerve within the fascial tunnel becomes progressively restricted
Under the combined load of obesity and prolonged standing, even without obvious trauma, the following can occur:
-
Chronic mechanical irritation of peripheral nerves
-
Gradual accumulation of neural tension
-
Final manifestation as localized foot pain
Therefore, the superficial peroneal nerve entrapment in this case is not an incidental event, but the result of:
Obesity and occupational prolonged standing
→ lower-limb biomechanical imbalance
→ peripheral nerve entrapment
This represents a complete causal chain.
3. Treatment Strategy
The treatment objective was clear:
To relieve mechanical entrapment of the superficial peroneal nerve within the fascial tunnel, while reducing ongoing load.
Treatment strategies included:
-
Releasing fascia and soft tissues around the nerve entrapment area
-
Reducing continuous mechanical irritation to the nerve
-
Emphasizing lifestyle-level adjustments, especially:
-
Avoiding prolonged uninterrupted standing
-
Optimizing work–rest cycles
-
Weight management as a core long-term intervention
-
The focus of treatment was not short-term pain suppression, but changing the conditions under which the nerve is chronically overloaded.
4. Clinical Insight
The key of Four-Level Thinking is not identifying “where the nerve is trapped,”
but understanding “why this person developed entrapment at this site.”
In this case, if one stops at the structural diagnosis of “superficial peroneal nerve entrapment” and ignores the patient’s body weight and occupational standing load, recurrence is likely.
Only by placing obesity and long-term load at the core of the etiological framework does diagnosis and intervention become complete.
#———————————————————————————————————————————————————#
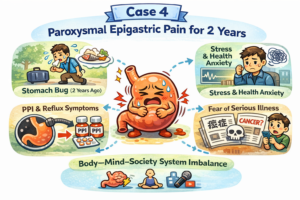
Case 4 | Paroxysmal Epigastric Pain for 2 Years
From an Acute Gastrointestinal Event to a Body–Mind–Society–Spirit System Imbalance
① Case Background
Patient:
Male, 30 years old, Kiwi, solid build, carpenter.
Timeline of the Condition
Approximately 2 years ago (initial event)
During overseas travel, the patient developed sudden nausea, vomiting, diarrhea, and abdominal pain, a presentation consistent with acute gastroenteritis / travel-related gastrointestinal disturbance.
After returning to New Zealand
The acute symptoms resolved, but residual issues persisted, including:
-
Ongoing gastric discomfort
-
Mild nausea
-
Heightened sensitivity to food
Subsequent GP management
The patient was prescribed proton pump inhibitors (PPIs) for approximately 3 months.
During PPI use, symptoms did not improve and gradually worsened.
After stopping PPI therapy
Over the following 6 months, gastrointestinal function gradually stabilized.
However, mild discomfort, occasional epigastric pain, and nausea remained.
The patient became extremely cautious with diet.
Past 2 months
Following a dietary trigger, symptoms recurred, including epigastric pain, nausea, and occasional diarrhea.
Although symptoms could settle spontaneously, psychological burden increased significantly.
Current acute episode (2 days prior to consultation)
The patient developed:
-
Severe abdominal pain
-
Marked nausea and vomiting
-
Diarrhea
Symptoms were intense and no longer tolerable.
Previous Investigations
Gastroscopy findings:
-
Gastric body, antrum, and duodenum essentially normal
-
No gastritis, no ulceration, no malignancy
-
Presence of fundic gland polyps
-
Lax lower esophageal sphincter
② Four-Level Thinking Analysis
Level 1 | Symptom Layer – What Is Observed
-
Paroxysmal epigastric pain
-
Nausea and vomiting
-
Diarrhea
-
High sensitivity to food stimuli
-
Recurrent, fluctuating symptom pattern
At this level, the case appears to be recurrent gastrointestinal discomfort, easily labeled as a “stomach problem.”
Level 2 | Functional / Organ Layer – Is the Stomach Itself Diseased?
The core question at this level is:
👉 Is there structural or organic damage to the stomach?
Key evidence:
-
Gastroscopy structurally normal
-
No inflammation, ulceration, or malignancy
-
Fundic gland polyps insufficient to explain symptom severity
-
Acid suppression with PPIs ineffective and even aggravating
Conclusion at this level:
This is not an organic gastric disease.
Continuing along a “gastritis / acid / GERD” pathway would lead only to repeated investigations and medication changes, without explaining symptom intensity or fluctuation.
Level 3 | Whole-System Layer – Gastrointestinal–Autonomic Dysregulation
When symptoms are viewed within the whole system, several features stand out:
-
Upper GI involvement (nausea, vomiting)
-
Lower GI involvement (diarrhea)
-
Triggered, episodic loss of control
-
Strong influence of attention, emotion, and worry on symptoms
This pattern is highly consistent with:
Dysregulation of the gastrointestinal–autonomic nervous system
In other words:
-
The stomach is not “damaged”
-
The intestines are not “infected”
-
The problem lies in system-level regulation
At this level, long-term PPI use did not correct regulation.
Instead, by suppressing gastric acid and altering the digestive environment and microbiota, it may have further weakened system resilience.
Level 4 | Spirit-Level (Psychological–Social–Information Environment)
This is the deepest and most critical layer of this case.
1️⃣ Psychological imprint of the initial acute event
A genuine, severe episode of acute gastroenteritis created a lasting fear of recurrence.
The patient became hypervigilant to any gastrointestinal sensation.
2️⃣ Modern disease information environment
In contemporary society:
-
Media, internet, and social platforms repeatedly emphasize
“stomach cancer,” “bowel cancer,” “serious illness in young people” -
Many individuals live in a state of cancer-related fear
This information environment is not neutral; it amplifies catastrophic interpretations of bodily sensations.
3️⃣ Behavioral adaptations becoming part of the problem
Over time, the patient developed:
-
Excessive dietary restriction
-
Avoidance of cold, spicy, or “stimulating” foods
-
Constant monitoring of gastrointestinal sensations
The result:
-
Chronic defensive autonomic state
-
Reduced adaptive capacity
-
Minor stimuli triggering disproportionate reactions
4️⃣ Key physical examination finding
-
No focal epigastric tenderness
-
Generalized abdominal tension and rigidity
This is a classic somatic manifestation of high autonomic tone associated with anxiety and vigilance.
③ Treatment Strategy
The therapeutic goal is not to “treat the stomach”, but to:
Restore global stability of the gastrointestinal–autonomic system
Core principles
-
Remove fear of organ damage
Clearly explain that the stomach “hardware” is intact and there is no serious disease. -
Avoid treatment at the wrong level
Discontinue unnecessary acid suppression and excessive interventions. -
Rebuild healthy life patterns
-
Regular daily rhythm
-
Post-work physical activity, exercise, stretching
-
Shift attention away from constant gut monitoring
-
-
Gradually restore dietary confidence
-
Avoid rigid dietary fear
-
Stop interpreting every discomfort as danger
-
The focus is system reset, not short-term symptom suppression.
④ Clinical Insight
This case illustrates that, in modern society, many conditions labeled as “gastric disease” are actually the result of:
Systemic dysregulation combined with disease-related fear
When clinicians remain confined to:
-
Organs
-
Investigations
-
Medications
Patients enter a cycle of:
-
More tests → more fear
-
More treatment → more chaos
-
Increasing system tension
The value of Four-Level Thinking lies in:
-
Identifying the correct level
-
Avoiding harm at the wrong level
-
Intervening where the system can truly recover
One-sentence summary
This is a body–mind–society–spirit integrated functional gastrointestinal disorder, initiated by an acute gastrointestinal event, maintained by systemic dysregulation, and amplified by modern information-driven disease fear.
Case 5|Ten Years of Low Back Pain — A Turning Point from “Pain-Spot Thinking” to “Force-Line Thinking”
① Case Background
The patient is a middle-aged male who had suffered from chronic low back pain for nearly ten years.
Over the past decade, he had tried various treatments including physiotherapy, massage, chiropractic adjustments, and acupuncture. Each intervention provided only temporary relief, and the pain would inevitably return. No clear structural pathology had ever been identified, and imaging studies were largely unremarkable.
By the time he presented to the clinic, the most striking feature was not the severity of pain itself, but the long-standing, treatment-resistant nature of the condition.
At first glance, this seemed like a typical case of chronic low back pain with no obvious red flags. However, it eventually became a pivotal case that marked a shift in diagnostic perspective.
② Four-Level Thinking Analysis
Level 1 — Symptom Layer: The Trap of “Where It Hurts”
On the surface, the case appeared straightforward. The patient complained of persistent low back pain localized to the lumbar region. Most previous treatments had focused directly on the painful area — loosening tight muscles, reducing local tension, or adjusting nearby joints.
This represents the most common clinical reflex: treating the pain where it appears. However, despite repeated interventions targeting the painful site, the symptoms kept recurring. This alone suggests that the true driver of the condition might lie beyond the pain point itself.
Level 2 — Functional Layer: Why Does the Pain Keep Returning?
At the functional level, the key question becomes: why does the relief never last?
The patient consistently experienced temporary improvement after manual therapy, but the pain gradually returned once normal activity resumed. This pattern strongly suggests that the underlying problem is not an acute injury, but a persistent biomechanical imbalance.
In other words, something in the patient’s movement system was continuously recreating the same mechanical stress.
Level 3 — Structural Layer: Seeing the Force Line
The turning point came during postural observation. From a lateral view, a clear structural pattern emerged:
-
Pronounced anterior pelvic tilt
-
Excessive lumbar lordosis
-
Weak abdominal wall support
-
Poor gluteal activation
This combination revealed a disrupted force transmission line through the trunk and pelvis. Instead of a balanced load-sharing system, the lumbar spine had been bearing disproportionate mechanical stress for years.
At this stage, the diagnostic focus shifted from isolated structures to force-line mechanics — understanding how global alignment shapes local pain.
The pain was no longer seen as a localized issue, but as the predictable outcome of a distorted biomechanical axis.
Level 4 — Deep Structural Insight: Why the Body Stayed This Way
The deepest layer of understanding lies not only in identifying structural imbalance, but in explaining its persistence.
Over many years, the patient had unknowingly adapted to a compensatory pattern: inactive gluteal muscles, under-engaged core stabilizers, and a pelvis locked in anterior tilt. These adaptations gradually became the body’s default motor program.
Once such a pattern becomes ingrained, passive treatments alone cannot restore balance. The body will repeatedly revert to the same structural configuration, reloading the lumbar spine and perpetuating the cycle of pain.
At this level, chronic pain is no longer viewed as a localized pathology, but as a long-standing structural habit encoded in the neuromuscular system.
③ Treatment Strategy
Once the primary structural axis is recognized, the treatment direction must fundamentally change.
The key is no longer “how much to release,” but “what needs to be rebuilt.”
Pure soft-tissue release can temporarily alter muscle tone, but posture will quickly pull everything back into its original pattern. Therefore, the therapeutic strategy must evolve from isolated release to a parallel model of release + reconstruction.
The core objectives are clear: reawaken gluteal activation, restore abdominal stability, and gradually guide the pelvis back toward a neutral position.
Treatment focuses on three coordinated components:
First, targeted soft-tissue release to reduce chronic compensatory tension, particularly in the lumbar extensors and hip flexors. This helps lower the mechanical load on the lumbar spine.
Second, structural re-education through movement retraining. Patients are guided to activate dormant muscle groups — especially the gluteal complex and deep core stabilizers — allowing the body to redistribute load more efficiently.
Third, long-term postural remodeling. Rather than chasing short-term pain relief, the emphasis is placed on gradually reshaping movement patterns so the spine is no longer forced into chronic overload.
Without this reconstruction phase, even the most refined manual therapy risks being overridden by the patient’s habitual posture.
④ Clinical Insight
This case represents a critical transition in clinical thinking — from chasing pain points to understanding force lines.
Many chronic low back pain cases are not driven by local tissue damage, but by long-standing distortions in global load distribution. If clinicians remain focused only on the site of pain, they may repeatedly miss the true driver.
The value of four-level thinking lies in expanding perspective. It allows us to move beyond symptoms, beyond local structures, and toward a deeper recognition of how the body organizes force and stability over time.
In essence, this is not merely a case of chronic low back pain. It is a reminder that long-standing pain often reflects long-standing structure — and that true resolution begins when we stop asking “where does it hurt?” and start asking “how is force moving through this body?”
 中文微信:nzacupunctureclinic
中文微信:nzacupunctureclinic
Leave a reply